Aaron had dreams of being a rock star.
As a Program Services Coordinator for Dungarvin Wisconsin since February 2010, I am responsible for supporting individuals with involved behavior support needs that are geared towards safety. Community integration can be limited for some of the individuals we support in these programs. Aaron came to Dungarvin in early 2011 with a long history of very involved behaviors and several failed placements. As I was first getting to know Aaron, one thing I quickly learned was that he had a passion for music – all types of music, but especially heavy metal. He had dreams of being a rock star. When I asked him why he wanted to be a rock star he replied, “I want to do this for my mom. Anything I could do to help her, I would do.”
After nearly two years of very remarkable progress in his program, Aaron’s team of professionals began to look for creative opportunities for Aaron to integrate into the community. The team came across an opportunity for individuals with developmental disabilities to be allowed access to a recording studio to record songs with a live band. This would be perfect for Aaron!

Collaboration
On July 18, 2013, Aaron and some members of his team made the journey to DNA Recording Studio in Madison, Wisconsin. Aaron’s dream was about to come true! When the group arrived at the studio, Aaron was excited at the opportunity but, at the same time, was completely relaxed and blended right in with everyone else. Aaron commented, “I always wanted to be in a band my entire life.” Aaron was able to hang out in the studio with the band and musical engineers. The band ran through the song they were going to record: Iron Man by Black Sabbath. Aaron was in Heaven! He really was going to be a rock star!
Mark Whitcomb, the recording studio owner, said this about Aaron: “He wasn’t shy or shocked about what was going on” and “he took direction well.” One of the professional musicians, Christian B., was very impressed with Aaron’s enthusiasm saying, “He was ready to go with whatever we said. Anything we suggested he was like ‘OK!’ It was awesome! Everybody should be like that. He has the kind of enthusiasm that is contagious.” Scott B., another of the professional musicians that was kind enough to work with Aaron, said Aaron had “a very positive attitude” and, “He was awesome! He owned it right away.”

Jam Session!
The video of Aaron recording his song turned out great! He sounded like a true rock star and even had some rock star moves. Mark made several copies of the video for Aaron. Aaron’s mother was first on the list to receive one.
For the individuals we serve, dreams may not come true every day, but on July 18, 2013, Aaron’s dream did. On that day, if only for a moment, Aaron was a rock star. On that day, Aaron was not a person with a developmental disability; he was one of the guys hanging out in the studio with the band. On that day Aaron made us all proud of the work we do at Dungarvin. Rock on!

Aaron’s Guitar Solo!
At Dungarvin Connecticut, we are transforming to apply clinical supports in a trauma-sensitive environment.

I sit quietly in the waiting room. Waiting always waiting; waiting on staff, waiting on my housemates, waiting to eat, waiting to take my meds, waiting for my ride, waiting for my appointment. Ugh! I rattle in my brain. I always was waiting. Over and over again all growing up, I waited and no one came home. I waited to eat. But, no one fed me. I waited in the dark. I heard the footsteps outside my door. But again, he came in and not my mom. Ugh! I can’t think about that. I can’t stand waiting. Why do they do this to me? Always have to wait; I can’t go, I can’t stay; I feel heat run through my body. I have to scream. I can’t. I ask my staff if we can leave. She says we have to wait. I rage. I go for her face. Punching, scratching. I can’t stop myself!
I am back in the chair; breathing heavily. Staff pin my arms against the chair. I can’t get up. I can’t move. She tells me to calm down and breathe. I can’t breathe. She keeps talking to me. I find it soothing. I can breathe. I am so sorry for scratching her.
The doctor will see me now. I hear the report about how aggressive I am. More meds ordered. Ugh. I am invisible. How long will I have to wait for someone to see me?
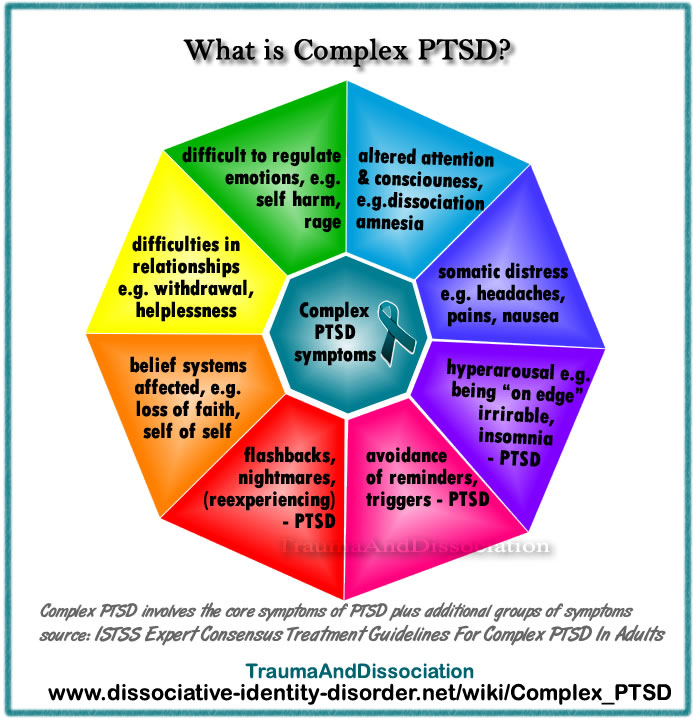
The National Child Trauma Stress Network defines the term complex trauma as “the problem of children’s exposure to multiple or prolonged traumatic events and the impact of this exposure on their development.” It may include neglect, physical and sexual abuse, domestic violence, and psychological abuse; it is chronic, begins in early childhood, and occurs within the primary care giving system. It can also begin prenatally with physical abuse to the pregnant mother, drug or alcohol abuse, and excessive cortisol production in response to significant and chronic stress that can negatively impact fetal development.
Only recently has the community of clinical practitioners considered those with intellectual disabilities appropriate candidates for counseling and other forms of psychotherapy, especially those with complex trauma. Challenging behaviors and demonstrations of emotional dis-regulation, previously regarded to function as “attention-seeking” or “task avoidance”, are now more widely recognized as signs and symptoms of emotional grief, mental health disorders, and trauma. Examples of such behaviors include self-abuse, aggression, property destruction, elopement, disrupted sleep; startle reflex, hyper-vigilance, refusals to engage in even pleasurable activities.
SAMSHA, in 2011, stated that an overwhelming percentage of the population has suffered “adverse events” that can be considered traumatic. According to Denise Valenti-Heim’s decades of clinical work and research, more than 90% of people with intellectual disabilities will experience some form of sexual abuse at some time in their lives. 49% will experience 10 or more abusive incidents.
To meet the needs and skills of those with intellectual disabilities who have survived trauma, some clinicians have adapted formal therapy models that are commonly employed to treat trauma, such as cognitive-behavior therapy, eye movement desensitization and reprocessing (EMDR), solution-focused brief therapy, symbolic interactive therapy, systematic desensitization, to name a few. These clinicians are exploring deeper layers of the psychological experience in an effort to address the illness and/or trauma; to provide the opportunity for actual healing. They transform the traditional model through a 6-point process to assist the individual learn, grow and develop the skills to handle stress, negotiate conflict, and attract and enjoy healthy relationships.
- Treat mental health issues through psycho-education about how the trauma impacted their sense of identity and worth, their rights to be safe, what is socially acceptable behavior, what is a healthy relationship, and how to effectively express feelings, needs, and preferences; develop self-confidence and positive self-image, and through psychopharmacology as necessary
- Address medical problems
- Minimize harm through trauma-sensitive programming and support
- Transform support system
- Educate the people in the individual’s life to minimize harm and PTSD triggers
- Participate in counseling
At Dungarvin Connecticut, we have embraced the transformation and recently opened our first home with a support system specifically focused on providing a trauma-sensitive healing environment in one of our CRS homes. This involved specific education and training, a redesign of behavior supports and IP development, and a paradigm shift in our perspective and approach to providing those supports.
Our team participated in a 2-day, complex trauma training, facilitated by the individual’s clinician, specifically focused on the individual the staff were to support. This was preceded by a 2-day, introduction to intellectual disabilities, mental health disorders, Applied Behavior Analysis (ABA) training, and teaching strategies.
Learning to identify feelings and express them effectively is a focus of this individual’s recovery because her challenges with these skills, has previously resulted in significant aggression, self-abusive behavior and elopement (as it is with many who have experienced trauma). While she participates in therapy with the clinician twice a week, one of the sessions takes place in her home (our program) to provide her the assistance she needs to apply what she learns in her office-based session. It is an opportunity for her to effectively express her needs, feelings, and preferences with both the staff and clinician present. With the support and guidance from the clinician, the individual is learning to tolerate increasing amounts of stress, work through misunderstandings, and self-advocate rather than self-destruct. Her first act of self advocacy was to request a change from the term, “staff”. She redefined our roles; we are “managers” or “workers” rather than “staff” as we are helping her to manage her life and we are working to support her.
This program is in its infancy and there is much more to learn from the experts and from the people we support in order to truly transform our support systems. We are dedicated to respecting and responding to the choices (and needs) of those we support; and are willing to do the work necessary to assist people with intellectual disabilities live with dignity and joy for as long as they will allow us to.
On December 20, 2006, a tragedy occurred when a fire broke out at one of the homes in Columbus, Ohio.
One of our valued direct service professionals, Peggy Porter, attempted to extinguish the fire and rescue the individuals receiving supports in the home, Tony B. and John C. All three were overcome by the heavy smoke. Tragically, the fire claimed the lives of Peggy and Tony. John was severely injured in the fire, but subsequently recovered. Every year since that terrible tragedy, Dungarvin Ohio celebrates and honors the memory of Peggy and Tony by holding a food drive in December.
Each year, our team sets a goal to exceed the previous year’s donations. We try to come up with new and exciting ways to motivate ourselves to give a little bit more than we gave the previous year. In December 2011, we raised $783 and collected 723 pounds of food. In December 2012, we raised $907 and collected 714 pounds of food.
For 2013, we decided to try something new. Rather than collect food, we focused all of our energy on raising money and decided to donate something just as valuable…our time. Although Mother Nature attempted to thwart our efforts by delivering a snow storm and causing all of the local schools to close, many members of the Ohio team, along with two NCO employees, braved the weather and headed to the Mid-Ohio Food Bank warehouse.

Dungarvin and other volunteers working hard at the Mid-Ohio Food Bank.

Jeff Sloat, Director and Cathy Rathburn, Special Projects Director, building boxes at the beginning of the assembly line.
Our volunteer group was assigned the task of making “care packages” for senior citizens in need. Along with a few volunteers from other organizations, we worked in an assembly line form, making boxes, packing them with non-perishable food items, sealing and then stacking the boxes. In just over two hours, we made and packed 565 “care packages”. As the volunteer coordinator at the food bank told us at the end of our shift, “565 seniors across the region get to eat because of your efforts here today.”

Lisa Fannin, Director, packing juice bottles into the care packages.

Crissy Hilgendorff, Program Director, ready to add cans of fruit to the care packages.

Adrienne Kennedy, Program Director, ready to add vegetables to the care packages.

Emily Joehlin, Program Director, breaking down empty food boxes.

Eilene Adkins, HR Specialist, breaking down empty food boxes.

Jennifer Gulley, Senior Director and Lori A., volunteer, ready to seal completed care packages.

Care packages ready to be distributed to senior citizens in need.
In addition, we were thrilled this year to deliver cash and checks to the Food Bank totaling $1,205! The Mid-Ohio Food Bank can purchase $11.00 worth of food for every dollar donated. It is exciting to know that our donation of $1,205 equated to $13,255 worth of food for additional people with needs in our region.
On that day, we left feeling like we had not only accomplished something wonderful, but that we proudly honored Peggy’s and Tony’s memories.

The Ohio team at the end of the volunteer shift at Mid-Ohio Food Bank.